Fariba Ahmadizar, PhD, of the department of epidemiology at Erasmus University Medical Centre, Rotterdam, the Netherlands, published a prospective, population based study showed risk of risk of type 2 diabetes with statin use. As it turns out in this study, the association between statin use and development of type 2 diabetes was strongest among those who were overweight or obese. So should everyone stop taking their statin? Certainly not. For those who are overweight or obese, reducing risk of type 2 diabetes through lifestyle changes and reducing insulin resistance is key. The major limitations to this study were lack of family history of type 2 diabetes, no hemoglobin A1 value or dose of statin. While this study is helpful, it certainly is limited in applying the results to general population. To learn more, please click below.
Let me begin by stating that I firmly believe the pricing of analog insulins must be addressed as this is vital issue affecting people living with diabetes. On to an interesting summary of a couple of studies on the use of human insulin in type 2 diabetes. A nice summary piece on a couple of recent studies published in JAMA on switching from analog to human insulin, and comparison of groups started on human versus basal analog insulin in persons with type 2 diabetes. The outcomes from these studies were positive for human insulin. To read this excellent summary, please click below.
Dapagliflozin (Farxiga, Xigduo) has an important label update – it can now be used in setting of moderate renal impairment (eGFR 45-59 mL/min/1.73 m2). This allows dapagliflozin to be used in a greater number of patients which is especially important in light of its cardiovascular benefit. The link below further describes this label update.
Another important label update is insulin glargine and lixisenatide injection (Soliqua 100/33) now having an indication for persons who had not achieved glycemic target on oral diabetes medication. Remember, Soliqua is a great alternative to basal bolus insulin regimen for persons with Type 2 diabetes. More details are provided in the link below.
In practice, I often find it helpful to use glucagon-like )GLP-1) receptor agonist in combination with sodium glucose cotransporter-2 (SGLT-2) inhibitor for type 2 diabetes as they tackle type 2 diabetes from different avenues. Using these two drug classes together creates synergy. Findings from a recent study of semaglutide, GLP-1 agonist, being added to SGLT-2 inhibitor (either alone or in combination with metformin or sulfonylurea) in persons with Type 2 diabetes who have inadequately controlled glucose improved glycemic control. Greater A1c and weight reduction were positive outcomes. Please click below to read this trial summary.
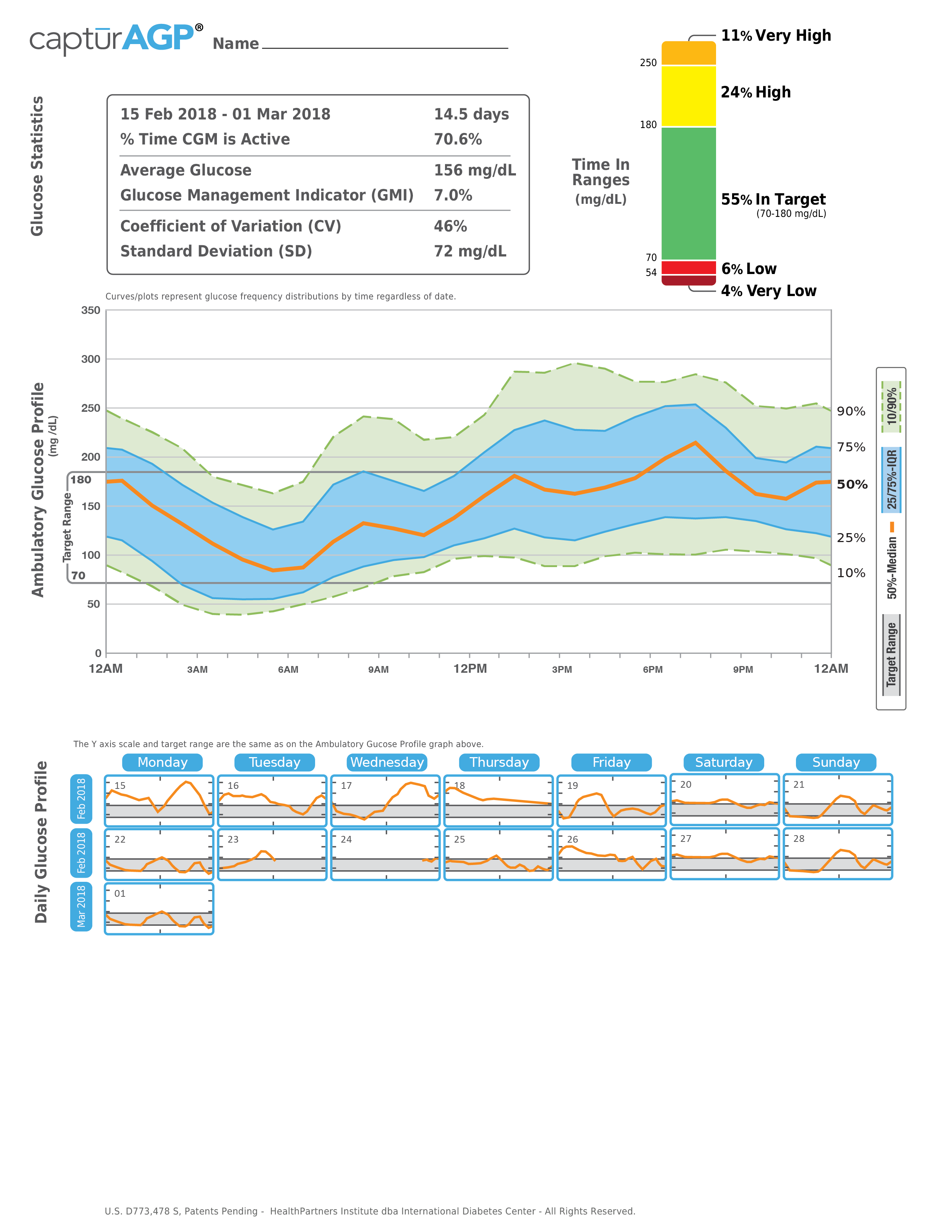
The International Diabetes Center has produced a great resource breaking down the ambulatory glucose profile for self monitoring of blood glucose (SMBG), continuous glucose monitoring (CGM), insulin pump and CGM, and closed loop pump and CGM. Below are a list of components of this profile.
Glucose statistics: average tests per day (SMBG ), percent time CGM active, average glucose (mean), GMI (glucose management indicator), CV (coefficient of variation), SD (standard deviation)
Time in range: time in target, low/very low, high/very high
Glucose profile: 24 hour picture of glucose; orange, blue and green zones
Daily glucose profile (SMBG and CGM): single day’s glucose pattern is represented in a box
Bolus insulin graph (pump and CGM, and closed loop pump and CGM): one graph of 24 hour insulin bolus doses
Insulin profile graph ( pump and CGM, and closed loop pump and CGM): shows basal insulin pump settings over 24 hour period
Below is a link with more detailed look at the AGP.
Following the ADA’s release of 2019 Standards of Care in Diabetes back in December 2018, AACE and ACE have now released their 2019 Consensus Statement on Comprehensive Type 2 Diabetes Management. This is a must read as much as ADA Standards of Care in Diabetes. Grab a cup of coffee or tie and sit in your favorite chair for a good read. The link is below.
There seems to be an app for everything these days in the diabetes world. So what makes FDA’s approval of an insulin phone app from Hygieia unique? This particular phone app is able to titrate individualized doses for all types of insulin regimens with the recommendations being delivered directly to the patient. This app with connect with any glucose meter and share data with the cloud. Hygieia currently has d-Nav insulin guidance service. Sounds interesting but I am sure that it has its pros and cons like all technologies. To learn more please click below.
Have every compared your finger stick glucose to your CGM glucose only to find s significant difference between the two values? So why? A physiologic time lag of glucose transport from the vascular to the interstitial space. Therefore, interstitial glucose readings (aka CGM readings) tend to lag finger stick glucose values by 5 – 10 minutes. It is even longer if glucose readings are changing rapidly. To learn more, click the link below to watch a short video.
As a diabetes educator, I have heard many people with diabetes say to me, “I did not want to come see you because I have bad control of my diabetes.” Some have even said, “I feel I have done everything that I can possibly do and I still have poorly controlled diabetes.” These statements reflect a sense of shame, blame, and frustration. My heart sinks every time I hear these statements. I want to yell it from the mountain tops a person with diabetes does not have to have it “all together” in order to see their diabetes educator or provider. Your diabetes educator and provider are here to support and empower you along this tough journey rather than place judgment on you. Yet, I also get that some diabetes educators and providers do judge people with diabetes based on what a person’s current A1C or blood values are.
So what are any alternatives to the term “control,” when used as a verb or adjective? “Manage” is an ideal alternative. So why? In reality, diabetes is a disease where the body no longer does what it is designed to do so “control” is really difficult to achieve in such a reality. By focusing on what the person is doing well, helps develop a structure to help the person build upon what that they are already doing well. It is not good or bad. Terminology that does not induce blame, shame or judgment is important. Have any of us ever benefited from being kicked when we were down or struggling? I certainly have not!
Control when used as a noun is often stated as good control,
bad control, or poor control. It takes
only a moment to realize that it creates a swinging pendulum where one feels
temporarily uplifted when they have “good control” and defeated when they are pronounced
to have “bad or poor control.” The reality of diabetes, like any other chronic
disease, is there are days where all is going as one would hope and then we
have those days where the feeling of what else could go wrong emerges. Alternatives for control should be based on
neutral words and on physiology. Terms
such as glycemic variability/stability/target/goal, blood glucose
levels/targets or A1C are more objective and based on biology.
In closing, a short story about Betty. I have been seeing Betty as her diabetes educator for a year. When I began seeing Betty, she would refer to herself as a “bad diabetic?” She would list off all of the self-management behaviors that she considered herself “failing” at. Betty really struggled to identify those behaviors that she had consistently performed. Finally, after about six months, Betty began to start off the conversation with behaviors that she consistently performed such as taking her insulin injections, following her eating plan and utilizing Freestyle Libre system for tracking glucose. Interestingly, Betty found herself building more positive behaviors upon other positive behaviors by shifting her focus from good or bad control.
Special thanks to
Jane Dickinson, Susan Guzman, Melinda Marynik, Catherine O’Brian, Jane
Kadohiro, Richard Jackson, Nancy D’Hondt, Brenda Montgomery, Kelly Close and
Martha Funnell who wrote Use of Language in Diabetes Care and Education